Coronary heart disease is common and patients may require coronary artery bypass grafting (CABG) surgery. The standard surgery requires open heart surgery and stopping of the heart temporarily.
What is coronary artery bypass grafting?
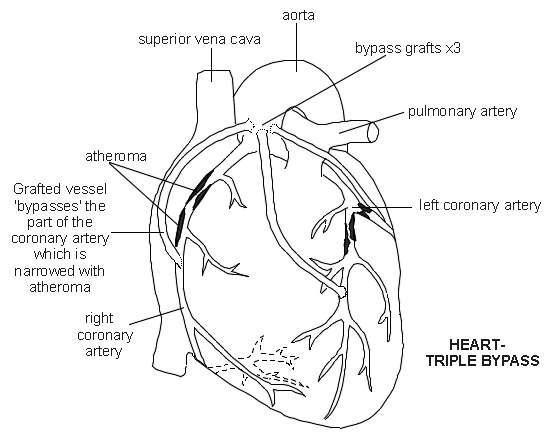
Coronary artery bypass grafting, called CABG for short (pronounced 'cabbage'), is a heart operation. In this blockages of the coronary arteries (supplying the heart muscle) are bypassed, usually using the patient's leg veins. It is major heart surgery and can be undertaken:
As the initial procedure.
As a repeat procedure.
After percutaneous coronary intervention (PCI) - also called 'stenting' - has failed.
What are the intended benefits of coronary artery bypass grafting?
The main reasons for carrying out a CABG procedure are to relieve symptoms of chest pain and to prevent further cardiac muscle from being starved of oxygen and the associated muscle death.
How is the decision to have coronary artery bypass grafting made?
Patients will already have had coronary angiography. This is a technique for taking special X-rays. A small tube (catheter) is inserted via the wrist or groin and dye is injected to look at the arteries in greater detail. The procedure is used to determine the extent of patients' heart disease.
A CABG procedure, rather than 'stenting' (percutaneous coronary intervention, or PCI) is likely to be undertaken when:
There is left main vessel disease.
There is complicated multiple vessel disease.
There is left ventricular dysfunction.
Diabetes mellitus is present.
Cases are usually discussed at a cardiac multidisciplinary team meeting, which consists of cardiologists, anaesthetists, cardiac nurses and cardiac surgeons. Other illnesses the patient has and surgical risk will also be discussed and be important in deciding on whether surgery is the right approach.
Patients who are high risk may have to stay in hospital and wait for urgent surgery.
What does coronary artery bypass grafting involve?
Patients will be anaesthetised with a general anaesthetic.
A mid-sternal incision (vertical incision through the breastbone) is made.
The grafts are commonly taken from the patient's leg veins; in some cases a chest wall artery may be used.
Most patients will need three or more grafts (common terms used are 'triple bypass' and 'quadruple bypass').
During a CABG procedure, the heart and lungs are temporary stopped and the blood bypassed through a machine to allow the grafts to be stitched in place:
A technique using a smaller incision has also been used - called minimally invasive direct coronary artery bypass (MIDCAB); however, it is only appropriate for certain cases and is not routinely available.
Operating without bypass is possible but CABG with temporary bypass is the standard.
Patients will usually need to be on the intensive care unit for 24 hours after the procedure.
They will usually have a chest drain inserted - a tube draining fluid from around the lungs. This will usually be removed 2-3 days later. They will also have a urinary catheter.
Patients can be ready for discharge after five days provided no complications occur.
What is the likely outcome of coronary artery bypass grafting?
CABG improves symptoms of angina, quality of life and exercise capacity.
Over 90% of patients will need a repeat CABG procedure after 10 years.
The risk of needing repeat surgery can be lessened by controlling the development of heart disease. This means stopping smoking, lowering blood pressure and cholesterol levels and controlling diabetes mellitus.
What factors worsen outcome after coronary artery bypass grafting?
Outcome (prognosis) may be affected by the following factors:
Increasing age.
Smoking.
Diabetes mellitus.
Overweight or obesity.
Other illnesses.
Left main stem disease, poor left ventricular function and multivessel disease.
If the operation was an emergency for unstable angina or shortly after a heart attack.
What are the complications of coronary artery bypass grafting?
Heart attack (myocardial infarction).
Acute kidney injury.
Ventricular arrhythmias.
Stroke occurs in 1-2%. Reducing handling of the aorta may reduce the risk. Pre-operative Doppler ultrasound scanning of the neck vessels is recommended in patients with a history of stroke or transient ischaemic attack:
In some people with significant 'furring' (plaque disease) of the main neck vessels, carotid artery revascularisation surgery at the same time as a CABG procedure may be performed.
Cognitive decline following CABG surgery has been reported in various studies. Most changes are mild and thought to reverse within the first few months after the operation.
Localised infection at the site of veins taken from the legs.
What follow-up is needed after coronary artery bypass grafting?
There will be surgical follow-up after discharge and then ongoing care with your general practitioner unless there are complications. Most patients will be referred on to cardiac rehabilitation.
Prevention of coronary heart disease is very important and will include:
Stopping smoking.
Use of long-term aspirin.
Use of an angiotensin-converting enzyme (ACE) inhibitor or an angiotensin-II receptor antagonist (AIIRA) - also called an angiotensin receptor blocker.
Use of beta-blockers.
Use of statins to achieve target cholesterol levels.